Bispecific Antibodies: How They Work and Their Role in Cancer Therapy
 Cynthia
8 min read
Cynthia
8 min read
In this Article
- What Are Bispecific Antibodies?
- Mechanism of Action (MOA) of Bispecific Antibodies
- Bispecific T Cell Engagers: A Powerful Subclass
- Types of Bispecific Antibody Formats
- Bispecific Antibodies in Cancer Therapy
- Bispecific Antibodies vs. CAR-T Therapy: Key Differences
- The Present and Future of Bispecific Antibodies for Cancer Therapy
- Final Thoughts
All of the products listed in AAA Biotech’s catalog are strictly for research-use only (RUO).
Key Learnings
- Bispecific antibodies have a dual-action mechanism, linking immune cells directly to cancer cells to trigger targeted tumor destruction.
- Advanced BiTE molecules redirect a patient’s T cells to attack cancer cells without requiring complex antigen presentation.
- FDA-approved therapies such as blinatumomab and teclistamab are already being used successfully to treat several blood cancers.
- Unlike CAR-T therapies, bispecific antibodies are manufactured in advance and available off-the-shelf, enabling faster and broader patient access.
- Ongoing research is expanding the use of bispecific antibodies beyond blood cancers and into difficult-to-treat solid tumors, including lung and breast cancer.
Cancer treatment has come a long way, from blunt-force chemotherapy to the precision-guided molecules of modern immunotherapy. One of the most compelling breakthroughs in recent oncology is the emergence of bispecific antibodies, a class of engineered proteins reshaping how we fight cancer at the molecular level.
If you're a patient, maybe a caregiver, or a researcher parsing the latest clinical data, we will break down what these molecules are, how they work, and why the scientific community is so excited about their potential.
What Are Bispecific Antibodies?
To understand bispecific antibodies, it helps to start with regular antibodies. Naturally produced by the immune system, antibodies are Y-shaped proteins, each with two identical "arms" that recognize and bind a single specific antigen. Monoclonal antibody drugs like trastuzumab (Herceptin) or rituximab are engineered versions of this single-target design.
A bispecific antibody breaks that mold entirely. It is an artificially constructed molecule with two distinct antigen-binding arms, each recognizing a different target. In cancer therapy, this typically means one arm latches onto a tumor-associated antigen on the cancer cell, while the other grabs an activating receptor on an immune effector cell — most commonly a T cell.
This dual-binding capability is the heart of what makes bispecific antibodies so powerful. They function as a molecular bridge, connecting the immune system directly to the tumor in a way that conventional antibodies or sometimes recombinant antibodies simply cannot achieve.
Mechanism of Action (MOA) of Bispecific Antibodies
So how do bispecific antibodies work at the cellular level? The core principle is enforced proximity. Cancer cells are notoriously skilled at evading immune surveillance; they mutate, downregulate surface markers, and suppress nearby immune activity. Bispecific antibodies overcome several of these evasion strategies in a single move.
Here is the step-by-step of the bispecific antibody mechanism of action:
Step 1: Dual Binding
One arm binds to a tumor-associated antigen (e.g., CD19, BCMA, or HER2) on the cancer cell surface. Simultaneously, the other arm binds to an activating receptor, typically CD3 on a nearby T cell.
Step 2: Immune Synapse Formation
This forced co-localization creates an artificial immune synapse: a tight junction between the T cell and the cancer cell that mimics the natural killing mechanism of cytotoxic T lymphocytes.
Step 3: T Cell Activation
The CD3-binding arm activates the T cell's killing machinery, triggering release of cytotoxic granules (perforin and granzymes) and pro-inflammatory cytokines directly at the tumor target.
Step 4: Tumor Cell Lysis
The cancer cell is destroyed. The T cell then disengages and remains available to engage and kill additional tumor cells, a process known as serial killing.
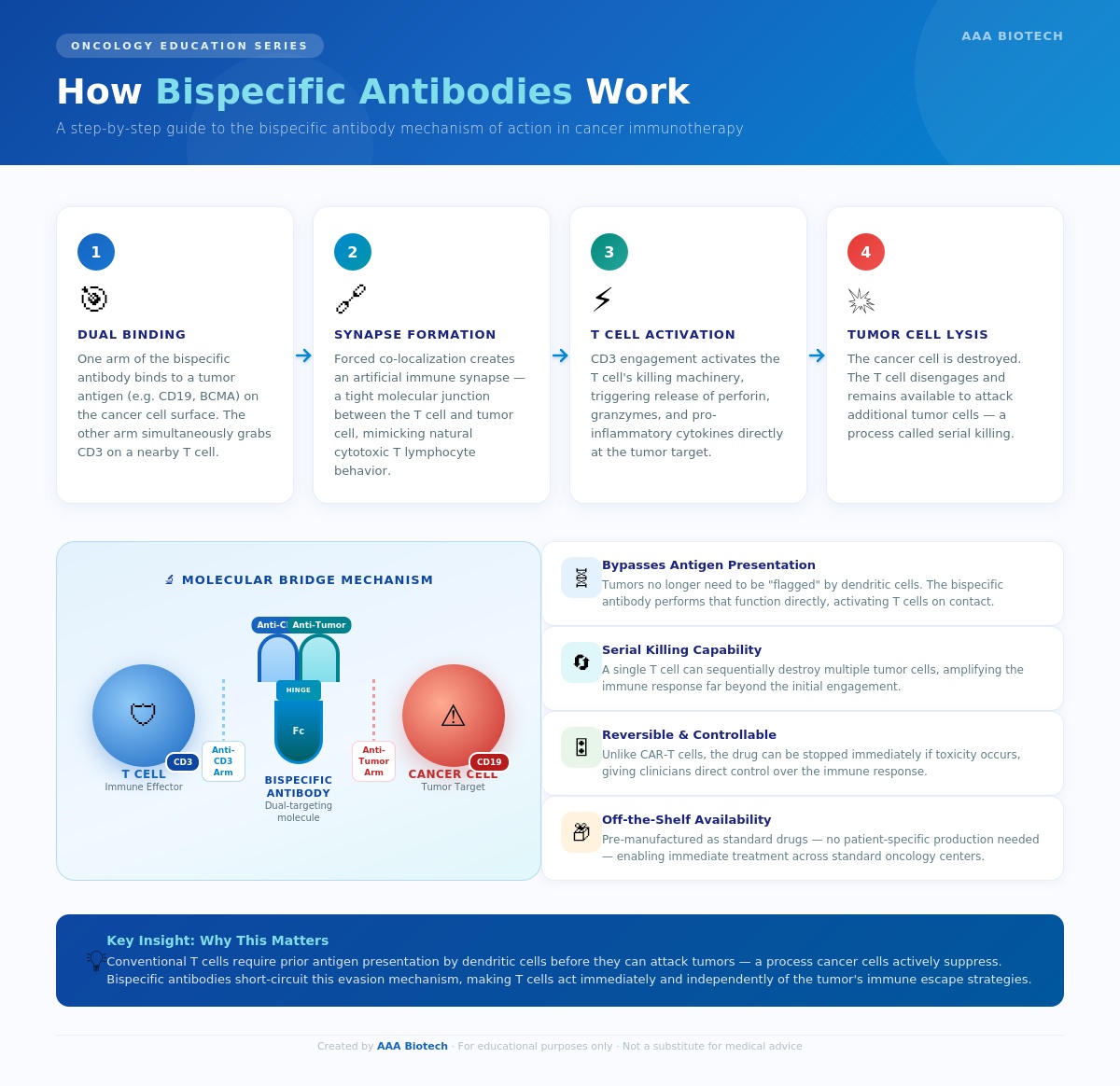
Note: This mechanism is particularly elegant because it bypasses the normal antigen presentation pathway. Tumor cells no longer need to be identified and flagged by dendritic cells before T cells can respond. Instead, the bispecific antibody acts as a bridge, directly connecting T cells to cancer cells and initiating an immune attack.
Bispecific T Cell Engagers: A Powerful Subclass
Among the various bispecific antibody formats, the bispecific T cell engager, abbreviated as BiTE, is the most clinically validated design. BiTEs are compact, flexible molecules that link an anti-CD3 arm (T cell targeting) with an antitumor antigen arm, without carrying the Fc region found in conventional antibodies.
This stripped-down architecture makes BiTEs highly potent, but also gives them a short half-life in circulation. Early BiTE drugs like blinatumomab require continuous intravenous infusion over 28-day cycles. To address this, next-generation "half-life extended" BiTE formats designed for subcutaneous weekly or biweekly dosing are now advancing through clinical development, significantly improving patient quality of life and treatment accessibility.
The BiTE platform has been particularly transformative in hematologic cancers, where circulating tumor cells are highly accessible to soluble antibody molecules in the bloodstream.
Types of Bispecific Antibody Formats
The field has produced a rich diversity of structural formats, including nanobodies and single-domain antibodies, each offering different pharmacokinetic and functional properties:
- BiTEs (Bispecific T cell Engagers): Small, Fc-free tandem single-chain constructs. High potency, short half-life.
Example: Blinatumomab.
- IgG-like bispecifics: Full-length antibodies with two different Fab arms. Longer half-life, broader immune effector function.
Example: Faricimab (ophthalmology), Amivantamab (oncology).
- DVD-Ig (Dual-Variable-Domain Immunoglobulin): Four binding domains in a single molecule for maximum targeting flexibility.
- Trispecific antibodies: An emerging next-generation format targeting three different antigens simultaneously, extending the logic of bispecific design into even more complex biology.
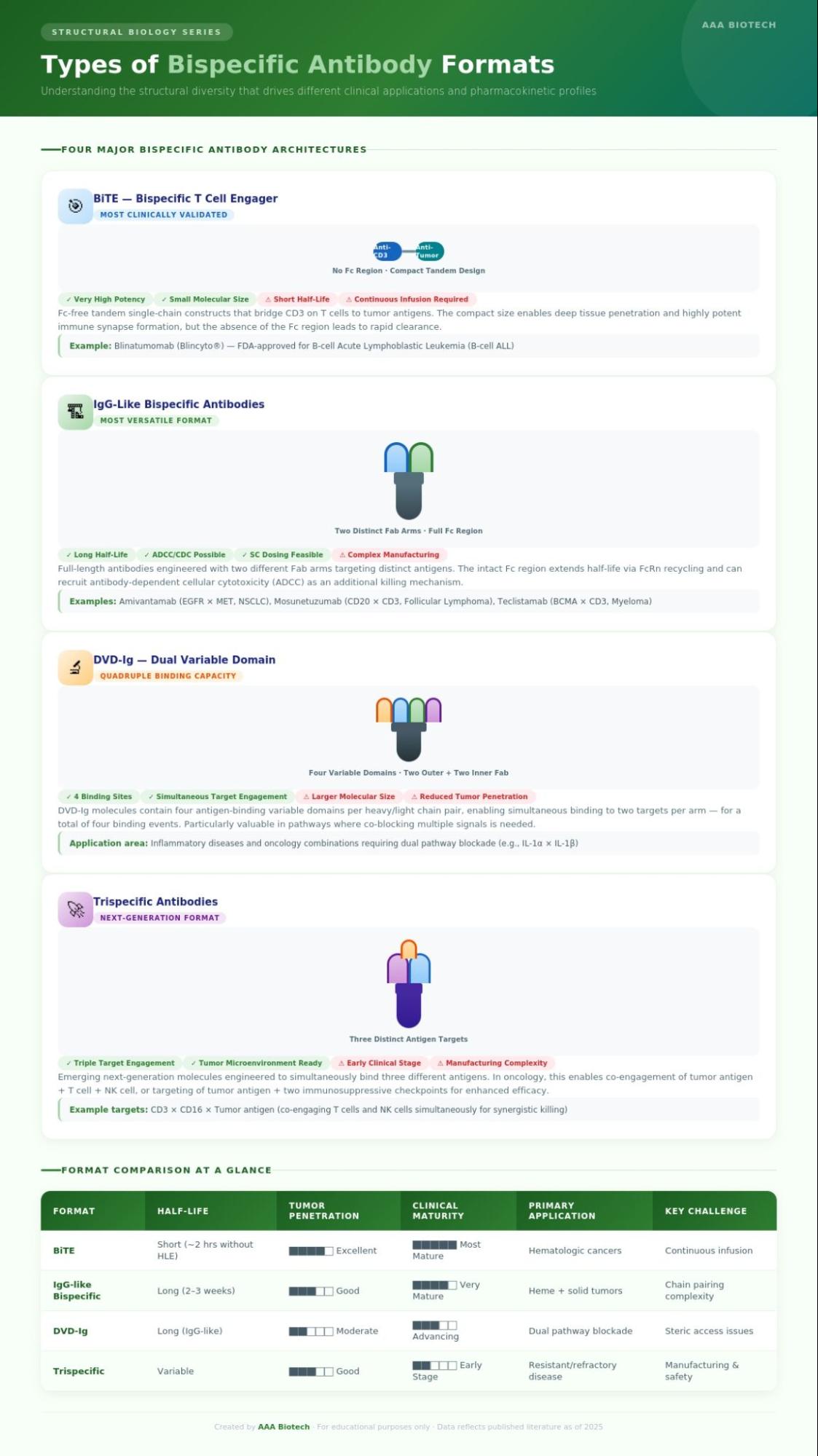
Each format involves deliberate trade-offs between half-life, tumor penetration, manufacturing complexity, and toxicity profile.
Bispecific Antibodies in Cancer Therapy
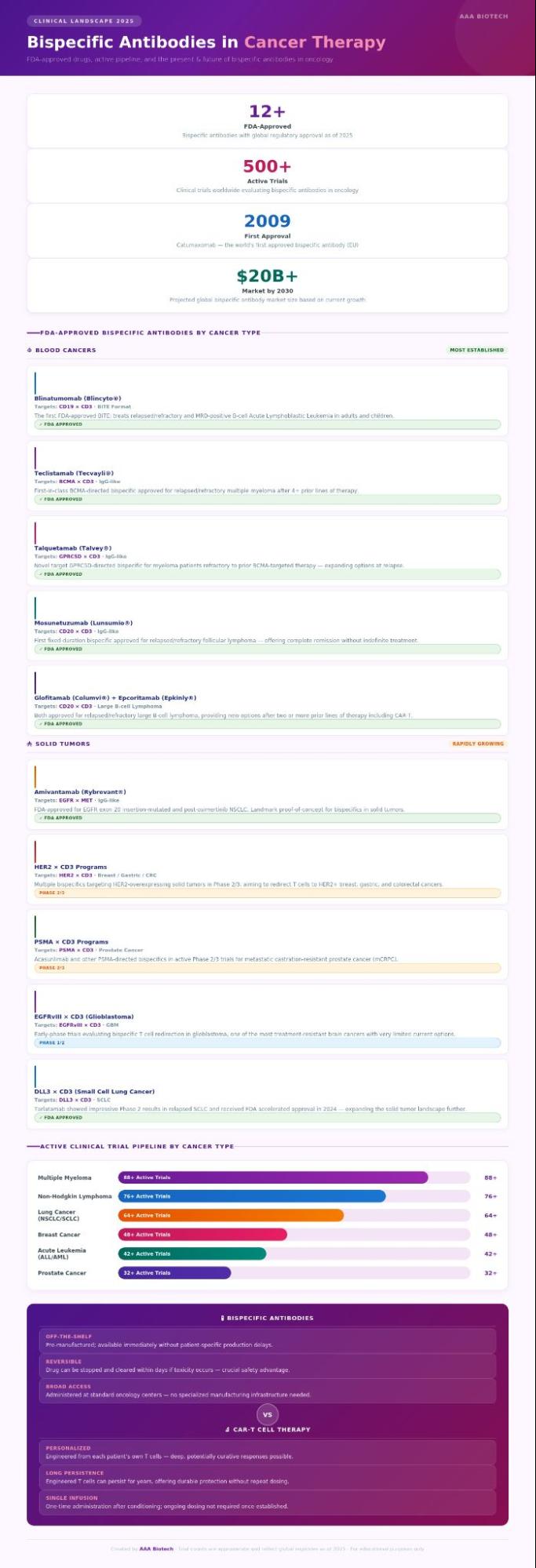
The clinical impact has been most dramatic in hematologic (blood) cancers, where multiple drugs are already approved and widely used.
Blood Cancers
- Acute Lymphoblastic Leukemia (ALL): Blinatumomab (CD19 × CD3) was the first BiTE approved by the FDA and has demonstrated strong outcomes in relapsed/refractory B-cell ALL, including patients with minimal residual disease who achieved morphologic remission but still harbored submicroscopic cancer cells.
- Multiple Myeloma: Teclistamab (BCMA × CD3), elranatamab (BCMA × CD3), and talquetamab (GPRC5D × CD3) have each demonstrated deep, durable responses in heavily pre-treated myeloma patients, including those refractory to prior BCMA-directed CAR-T therapy.
- Non-Hodgkin Lymphoma: Mosunetuzumab (CD20 × CD3) became the first fixed-duration bispecific antibody approved for follicular lymphoma. Glofitamab and epcoritamab are now also approved for relapsed/refractory large B-cell lymphoma.
Solid Tumors
Extending bispecific antibodies into solid tumors presents steeper challenges, with denser tumor microenvironments, heterogeneous antigen expression, and immunosuppressive barriers all complicating response. Despite this, active programs are generating real clinical signals in:
- EGFR-mutated non-small cell lung cancer — amivantamab (EGFR × MET) is already FDA-approved
- HER2-positive cancers (breast, gastric, colorectal)
- Prostate cancer (PSMA × CD3 bispecifics in Phase II/III)
- Glioblastoma (EGFRvIII × CD3 programs in early trials)
Bispecific Antibodies vs. CAR-T Therapy: Key Differences
Both modalities represent landmark advances in cancer immunotherapy, but they differ in critical ways:
| Feature | Bispecific Antibodies | CAR-T Cell Therapy |
|---|---|---|
| Manufacturing | Standard pharmaceutical production | Personalized, patient-specific |
| Time to Treatment | Immediate (off-the-shelf) | 3–6 weeks of manufacturing |
| Administration | IV infusion or SC injection | Single infusion post-conditioning |
| Reversibility | Drug can be stopped | T cells persist long-term |
| Accessibility | Broad; standard oncology centers | Limited specialized centers |
| Toxicity Profile | CRS, ICANS (generally milder) | Severe CRS and neurotoxicity possible |
Leading oncologists consistently frame these as complementary, not competing, tools. The future of cancer care will likely involve deploying both strategically, based on individual patient and disease characteristics.
The Present and Future of Bispecific Antibodies for Cancer Therapy
The present and future of bispecific antibodies for cancer therapy are extraordinarily promising. As of 2026, more than a dozen bispecific antibodies hold global regulatory approval, and several hundred clinical trials are actively enrolling.
Key trends shaping what comes next:
- Combination regimens: pairing bispecific antibodies with checkpoint inhibitors, lenalidomide, or daratumumab to deepen and extend responses.
- Earlier lines of therapy: moving from relapsed/refractory settings toward frontline treatment protocols, where curative intent becomes more realistic.
- Solid tumor breakthroughs: continued engineering innovation to penetrate and reshape the immunosuppressive tumor microenvironment.
- Conditional activation ("masked" bispecifics): molecules designed to activate only within the tumor microenvironment, maximizing on-target efficacy while reducing systemic toxicity.
- Subcutaneous delivery: simplified dosing schedules, reducing infusion burden, and expanding outpatient treatment options.
The convergence of structural biology, protein engineering, and translational immunology is accelerating the pace of innovation in this space at a rate few could have predicted even five years ago.
Final Thoughts
Bispecific antibodies represent one of the most dynamic and clinically impactful innovations in modern oncology. By engineering molecules that simultaneously engage tumor cells and immune effectors, researchers have created a platform that is already saving lives and has the potential to transform treatment across a much broader range of cancer types.
As the science matures and novel formats emerge, the field will continue to expand what is possible for patients who have run out of conventional options. The journey from bench to bedside for these molecules has been remarkable, and, by all indications, is only beginning.
Word of Advice from AAA’s Research Team: This article is intended for educational purposes only and does not constitute medical advice. Consult a qualified oncologist or healthcare professional for personalized treatment guidance.
Faq's
What is a bispecific antibody in simple terms?
A bispecific antibody is an engineered protein that binds to two different targets at the same time, typically one on a cancer cell and one on an immune cell. This forces the immune cell into direct contact with the cancer cell, triggering its destruction. Think of it as a molecular matchmaker that engineers a meeting between your immune system and a tumor.
Are bispecific antibodies a form of immunotherapy?
Yes. Bispecific antibodies are classified as cancer immunotherapy. Rather than directly poisoning cancer cells (as chemotherapy does), they work by redirecting and activating the patient's existing immune system, specifically T cells, to recognize and eliminate tumor cells.
What cancers are currently treated with FDA-approved bispecific antibodies?
FDA-approved bispecific antibodies currently treat several blood cancers: B-cell acute lymphoblastic leukemia (blinatumomab), multiple myeloma (teclistamab, talquetamab, elranatamab), and non-Hodgkin lymphoma (mosunetuzumab, glofitamab, epcoritamab).
Amivantamab is approved for EGFR-mutated non-small cell lung cancer, a significant milestone for solid tumor applications.
What side effects should patients expect from bispecific antibodies?
The most common side effects include cytokine release syndrome (CRS) — an immune overreaction causing fever, fatigue, and low blood pressure, and immune effector cell-associated neurotoxicity syndrome (ICANS). These are typically manageable with prompt medical intervention and are generally less severe than side effects seen with intensive chemotherapy or some CAR-T therapies. Patients are closely monitored, especially during early treatment cycles.
How are bispecific antibodies different from CAR-T cell therapy?
The fundamental difference is manufacturing. CAR-T therapy requires collecting the patient's own T cells, genetically engineering them in a laboratory over several weeks, and reinfusing them. Bispecific antibodies are pre-manufactured drugs, which are ready off-the-shelf, making them faster to administer, widely available at standard oncology centers, and easier to stop if side effects occur. Both therapies have a role; they are increasingly used together or sequentially rather than as alternatives.
Lead Clinical Research Coordinator (LCRC)
Cynthia Lee is the President of AAA Biotech and specializes in understanding highly validated and characterized monoclonal/polyclonal antibodies, recombinant proteins, and ELISA kits.