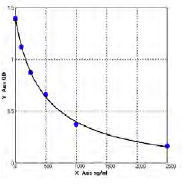
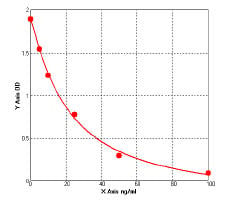
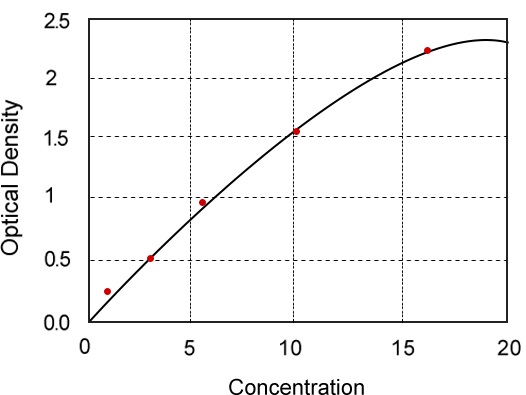
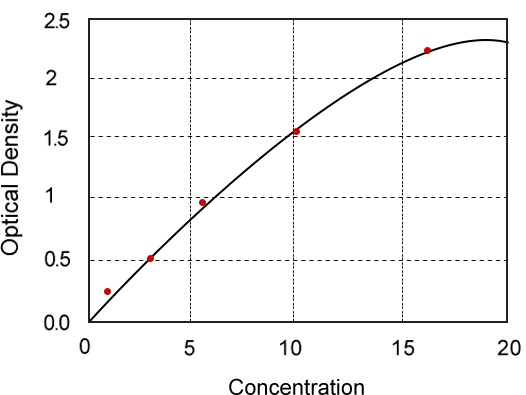
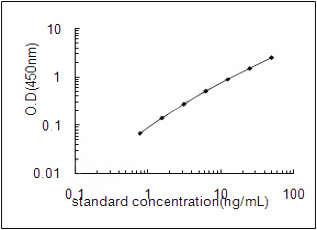
 Standard Curve (Sample)
Standard Curve (Sample)
HSA kit
TRANSIL HSA Binding Kit
Synonyms
HSA; N/A; TRANSIL HSA Binding Kit; HSA kit
Samples
Human serum albumin
Preparation and Storage
Store at -20 degree C
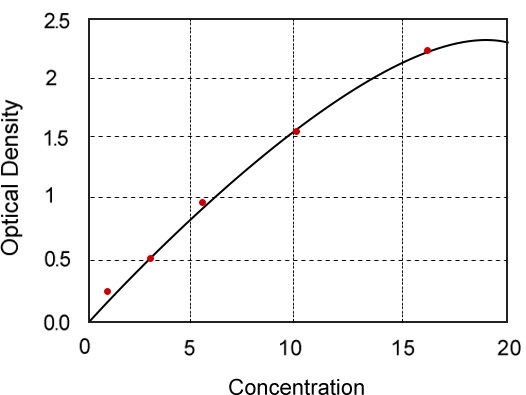
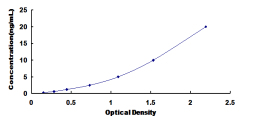
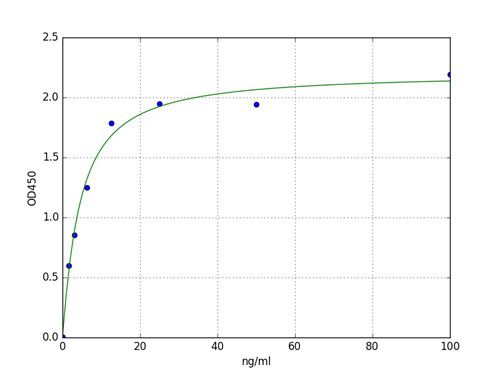
Standard Curve (Sample)
Standard Curve (Sample)
Related Product Information for HSA kit
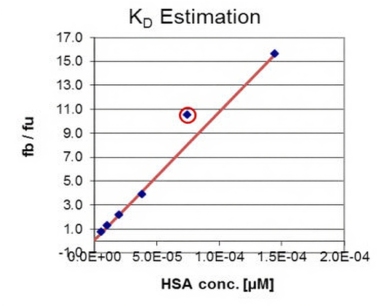
Background: It is commonly accepted that only the unbound fraction (fu) of a drug can penetrate cell membranes and exert its pharmacological effect or become available for elimination. Many drugs, especially lipophilic compounds, bind to circulating plasma proteins, such as human serum albumin (HSA), alpha1-acid glycoprotein (AGP), globulins, and lipoproteins. Among these proteins, HSA and AGP are the most important for the reduction of the exposure to xenobiotics because of their ability to bind a large array of structurally unrelated drugs in distinct binding sites (Kremer et al., 1988; Peters, 1996). Human serum albumin (HSA) is the most abundant protein in blood plasma. It is synthesized in the liver and concentrations in healthy subjects normally range between 35 and 60 g/L with an average of 42 g/L (Peters, 1996). HSA comprises 60% of the total plasma proteins. Its main physiological function is to bind and carry endogenous anions, with longchain fatty acids. Two high affinity binding sites have been proposed in subdomains IIA (also known as Sudlow's site I or warfarin site) and IIIA (also known as Site II or benzodiazepine site) of HSA. These comprise highly elongated hydrophobic pockets with charged lysine and arginine residues near the surface that interact with polar ligand parts. In contrast to AGP, HSA blood levels are much more stable. Hyperalbuminemia (HSA > 55 g/L) is seldom seen in the absence of dehydration whereas hypoalbuminemia is the more common condition resulting from malnutrition or liver disease with serum albumin levels dropping to 20-23 g/L (Peters, 1996). Human AGP, also called orosomucoid, is a small acute-phase glycoprotein (about 40 kD), synthesized mostly by hepatocytes and is present in the plasma of healthy subjects at concentrations that range from 0.36 to 1.46 g/L with a mean of 0.77 g/L (Blain et al., 1985), accounting for about 1% to 3% of total plasma protein. AGP exhibits a sequence homology of 75% with immunoglobulins (Schmid et al., 1973) and functions as a carrier protein for basic and neutral lipophilic endogenous compounds such as steroid hormones or xenobiotics (Kremer et al., 1988). AGP levels can vary considerably in response to disease with values up to 2.8 g/L observed in patients with viral or bacterial infections (Voulgari et al., 1982) or 10-fold differences (0.3-3 g/L) being found in cancer patients (Jackson et al., 1982). Moreover, AGP is expressed at lower levels in the fetus (0.15 g/L) than the mother (0.5 g/L), resulting in a higher free fraction of drugs, e.g. propranolol and lidocaine, in neonatal blood than in maternal blood (Wood M & Wood AJ, 1981). It has been shown that plasma levels of AGP inversely correlate with the fu of alprenolol (Piafsky & Borga, 1977), docetaxel (Loos et al., 2003), disopyramide (Bredesen & Kierulf, 1986), imipramine (Piafsky & Borga, 1977), and propranolol (Piafsky et al., 1978). Significant differences in the fu of disopyramide between population of Black (Johnson & Livingston, 1997), Chinese (Zhou et al., 1990) and White backgrounds suggest differences in AGP levels. In a recent clinical study, AGP could be identified as an independent predictor for a clinical endpoint, i.e. survival in patients with non-small cell lung cancer treated with docetaxel (Bruno et al., 2003). Given the clinical relevance of fluctuation in the fu altering drug disposition (Summerfield et al., 2006), active transport (Bow et al., 2006), drug-drug interactions (Christensen et al., 2006) and drug efficacy, especially in the field of chemotherapy of infectious diseases (Boffito et al., 2002; Zhang et al., 1999) there is an increased understanding that binding to plasma proteins should be investigated in the early stages of the drug discovery process. Unfortunately, existing methods for determination of plasma protein binding have low capacity and/or high cost and lack standard evaluation procedures (for a review, see Boffito et al., 2003). Conventional methods to determine plasma protein binding comprise equilibrium dialysis, ultrafiltration, and ultracentrifugation (Sebille, 1990), ideally using plasma samples of pooled healthy donors, usually with no control over HSA and AGP levels. High throughput methods have been described for plasma equilibrium dialysis combined with liquid chromatography/ mass spectrometry (LC-MS/MS) analytics (Wan & Rehngren, 2006). Notably, the resolution of these methods is limited, particularly when examining drugs that are highly bound to plasma proteins. These conventional methods require highly sensitive analytical techniques that exhibit a linear range of more than two orders of magnitude such as LC-MS/MS or the use of radiolabeled compounds to resolve plasma protein binding of compounds with fu-values smaller than 0.01. Given the above constraints for the determination of plasma protein binding, the TRANSIL HSA and TRANSIL AGP Assay kits were developed and validated employing a novel method that overcomes these limitations and addresses the problem of varying HSA and AGP levels. To overcome the analytical limitations, when examining drugs that are highly bound to plasma proteins, the TRANSIL HSA and TRANSIL AGP Binding assays allow KD-values to be determined by titrating different subphysiological concentrations of HSA and supraphysiological concentrations of AGP against a constant drug concentration.
Principle of the Assay: The principle of the TRANSIL HSA Binding Kit is to assess the affinity of test compounds to the human plasma protein albumin (HSA). Albumin binding is determined by incubating a fixed concentration of drug candidate with varying concentrations of albumin immobilized on silica beads. A total of 8 wells of a tube unit are used to determine the plasma protein binding for each compound (Figure 1). Six wells contain HSA covered silica beads, while two serve as references to account for non-specific binding and contain buffer only. Using the spreadsheet and algorithms supplied with the kit, the affinity to albumin is calculated from remaining free compound concentration in the supernatant of each well. Any of the available detection systems, such as HPLC, LCMS, etc can be used for quantification, as long as it can quantify uM concentrations in volumes of 50 ul or less.
Principle of the Assay: The principle of the TRANSIL HSA Binding Kit is to assess the affinity of test compounds to the human plasma protein albumin (HSA). Albumin binding is determined by incubating a fixed concentration of drug candidate with varying concentrations of albumin immobilized on silica beads. A total of 8 wells of a tube unit are used to determine the plasma protein binding for each compound (Figure 1). Six wells contain HSA covered silica beads, while two serve as references to account for non-specific binding and contain buffer only. Using the spreadsheet and algorithms supplied with the kit, the affinity to albumin is calculated from remaining free compound concentration in the supernatant of each well. Any of the available detection systems, such as HPLC, LCMS, etc can be used for quantification, as long as it can quantify uM concentrations in volumes of 50 ul or less.
Product Categories/Family for HSA kit
Customer Reviews
Loading reviews...
Share Your Experience
Similar Products




Product Notes
The HSA (Catalog #AAA60729) is a Kit and is intended for research purposes only. The product is available for immediate purchase. It is sometimes possible for the material contained within the vial of "HSA, Kit" to become dispersed throughout the inside of the vial, particularly around the seal of said vial, during shipment and storage. We always suggest centrifuging these vials to consolidate all of the liquid away from the lid and to the bottom of the vial prior to opening. Please be advised that certain products may require dry ice for shipping and that, if this is the case, an additional dry ice fee may also be required.Precautions
All products in the AAA Biotech catalog are strictly for research-use only, and are absolutely not suitable for use in any sort of medical, therapeutic, prophylactic, in-vivo, or diagnostic capacity. By purchasing a product from AAA Biotech, you are explicitly certifying that said products will be properly tested and used in line with industry standard. AAA Biotech and its authorized distribution partners reserve the right to refuse to fulfill any order if we have any indication that a purchaser may be intending to use a product outside of our accepted criteria.Disclaimer
Though we do strive to guarantee the information represented in this datasheet, AAA Biotech cannot be held responsible for any oversights or imprecisions. AAA Biotech reserves the right to adjust any aspect of this datasheet at any time and without notice. It is the responsibility of the customer to inform AAA Biotech of any product performance issues observed or experienced within 30 days of receipt of said product. To see additional details on this or any of our other policies, please see our Terms & Conditions page.Item has been added to Shopping Cart
If you are ready to order, navigate to Shopping Cart and get ready to checkout.